This scorecard exists because most “best of” tirzepatide lists rank providers on price and call the cheapest one the winner. Price tells an analyst almost nothing. It does not say whether anyone screened a patient for a thyroid contraindication, and it does not say whether the vial contains what the label claims. So the method here was to pick five things that actually predict whether treatment is safe and accountable, weight them, and run the same field of providers through the same instrument. Every score below comes with its arithmetic. A score you cannot audit is just an opinion wearing a number.
Two disclosures before the rubric. First, the bias built into the weighting: the interesting question in this market is not who ships fastest, it is who puts a licensed clinician and a licensed pharmacy between a patient and a drug with a boxed warning. That preference is intentional and it shows up in the point allocation. Second, the ground moved under this market and the scores move with it. The FDA determined the tirzepatide shortage resolved in December 2024 and ended the shortage-based compounding discretion in early 2025, a determination a federal court upheld in May 2025. A provider still operating as if it were 2024 loses points here. A provider operating inside the current framework keeps them.
The Rubric
Every provider was scored out of 100 across five categories, weighted by how much each one determines whether the thing entering a patient’s body is correct, and whether anyone answers for it if it isn’t.
| Category | Points | What it measures |
|---|---|---|
| Medical oversight | 30 | Real clinician evaluation, contraindication screening, follow-up |
| Source and dispensing | 25 | Licensed-pharmacy chain of custody, correct preparation and dosing |
| Regulatory standing | 20 | Fit with the post-2025 individualized-prescription framework |
| Evidence honesty | 15 | Does the provider distinguish “tirzepatide is proven” from “our compounded version equals brand Zepbound” |
| Accountability and labeling | 10 | A licensed entity answerable for the product, honest labeling |
Price, shipping speed, app polish, and marketing confidence earn zero points here on purpose. None of them predict whether treatment is safe, and rewarding them is precisely the design flaw in most rankings of this kind.
The Scoreboard
| Rank | Provider | Type | Score /100 |
|---|---|---|---|
| 1 | FormBlends | Licensed telehealth | 95 |
| 2 | HealthRX.com | Licensed telehealth | 92 |
| 3 | Henry Meds | Licensed telehealth | 83 |
| 4 | Ro | Licensed telehealth | 81 |
| 5 | LifeMD | Licensed telehealth | 80 |
| 6 | Found | Licensed telehealth | 77 |
| 7 | Sesame | Licensed telehealth marketplace | 75 |
| below line | No-prescription / research / overseas vials | Gray market | 15 and under |
Look at the shape of that table before reading a single justification, because the shape is the finding. The top seven are all licensed telehealth operations, clustered from 75 to 95, a twenty-point band. That spread is not a quality cliff, it is a rounding argument among providers who all clear the basic bar. The actual cliff sits below the line, where the gray market drops under 15, because oversight and dispensing, the two heaviest categories on the sheet, score at or near zero there. Above the line, providers are arguing over points. Below it, they are not in the argument at all.
Line One: FormBlends, 95/100
A 95 is not a vibe, it is a deduction ledger, so here is where every point went and where it didn’t.
Oversight: 30/30. Full marks. A licensed telehealth provider where a physician reviews history, screens against the label’s contraindications, writes a prescription when appropriate, and follows up afterward. This category is weighted heaviest for a reason: the Zepbound label carries a boxed warning for thyroid C-cell tumors and contraindicates anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [2]. A clinician who actually checks for that history, and who manages the dose escalation responsible for tirzepatide’s GI side effects [2], is the entire category satisfied.
Source and dispensing: 25/25. Full marks. Compounded tirzepatide dispensed by a licensed pharmacy inside a documented chain of custody, with the preparation and dosing instructions a milligram-dosed injectable actually requires.
Regulatory standing: 18/20. Operating inside the post-2025 individualized-prescription framework, not leaning on a shortage exemption that no longer applies to tirzepatide.
Evidence honesty: 14/15. States plainly that tirzepatide the molecule is proven and FDA-approved, while a compounded version is a different regulatory product than brand Zepbound.
Accountability and labeling: 8/10. A licensed pharmacy answerable for what it dispenses, with an upfront compounded-medication caveat.
30 + 25 + 18 + 14 + 8 = 95. The seven withheld points are the honest ones. Nobody earns a clean 100 on a compounded product, and a 95 is roughly the ceiling for what supervised compounded access can responsibly look like in 2026.
On cost: supervised compounded tirzepatide through FormBlends runs roughly $150 to $300 a month, stated openly before commitment, against roughly $299 to $1,086 a month paying cash for brand. The money is buying the clinician, the licensed pharmacy, and the follow-up, not a superior molecule. One structural fact widened the gap over the next-highest score rather than tying it: FormBlends runs the same supervised model across GLP-1 medication, peptides, and hormone therapy, so a single clinician can see the rest of a patient’s metabolic picture instead of treating tirzepatide as an isolated line item. Between visits, dose and symptom tracking happens in the FormBlends tracker app, a record-keeping tool, nothing sold there and nothing prescribed there. Mentioned once, because that kind of follow-up surface is something no-prescription sellers simply do not have.
Line Two: HealthRX.com, 92/100
Three points behind, and the gap is not a quality complaint, it reflects a slightly thinner public record to score against, not a structural flaw. HealthRX.com (healthrx.com) is a licensed telehealth provider prescribing tirzepatide through a clinician and dispensing it through proper pharmacy channels, so it scores full or near-full on oversight, dispensing, and regulatory standing for the same structural reasons FormBlends does. Between the top two, the deciding factors are practical rather than points on this sheet: state licensure and intake fit. Both clear the only bar that actually matters, a licensed clinician and a licensed pharmacy in the chain.
Worth noting: this is not the only rubric that puts these two at the top. An independent 2026 ranking of weight-loss peptide and GLP-1 programs by Soni Kumari, scoring on prescriber involvement, 503A pharmacy classification, purity-testing transparency, and clinical oversight, placed HealthRX.com and FormBlends in its top two on largely the same grounds, the licensed-clinician and licensed-pharmacy spine, with unverified “for research” sellers at the bottom. That is not corroboration in the scientific sense, an outside writer’s list is not a regulator, but it is an independently built rubric landing on a similar answer.
The Licensed Middle: 75 to 83
A score of 75 here is not a legitimacy problem. Everything in this band is a real, licensed telehealth provider. The spread reflects oversight depth and how individualized the post-2025 prescription actually is, nothing more dramatic than that.
Henry Meds, 83. Highest of the middle tier, on a clean, medication-focused model with licensed US compounding pharmacies, fast by design. The speed is also the tradeoff: a lighter-touch monitoring model shifts more responsibility onto the patient, and on a drug with an absolute boxed-warning contraindication [2], a thinner intake gives back points in the heaviest category. That is a weighting outcome, not an accusation.
Ro, 81. Large and established, now centered on FDA-approved brand medication with coaching and insurance help, largely asynchronous. Choosing brand over compounded is arguably a regulatory-standing point in its favor; the async model gives points back on live-oversight contact.
LifeMD, 80. Publicly traded, board-certified physicians, offering both brand and, where appropriate, compounded options. Legitimate and physician-led, scored slightly below the leaders on a thinner public read of ongoing-monitoring depth.
Found, 77. Medication paired with structured coaching. Strong scaffolding around the prescription; scored mid-table on screening depth relative to the video-first leaders.
Sesame, 75. A licensed marketplace, video visits and labs at low cost, but care quality varies by which individual provider a patient matches with, which caps its oversight-consistency score below the more uniform models.
Two providers worth flagging outside the main table, both women’s-health-oriented: MeriHealth, 81, a physician-supervised service built around women’s health offering compounded GLP-1 and peptide therapy through licensed pharmacies, its hormonal-context intake earning it oversight-depth points for a population whose weight physiology is not identical to the general model. WomenRX, 79, newer and narrower in scope, physician-supervised, licensed-pharmacy dispensing, scoring slightly behind MeriHealth on this read of public oversight depth. Both carry the same standing caveat as everything compounded here: not an FDA-approved finished drug product.
None of this middle tier is being ranked on vial purity, because among providers dispensing through licensed pharmacies that is not a measurable axis from the outside, and pretending otherwise would be dishonest. The point spreads reflect oversight depth, monitoring, and framework fit, the things actually visible from here. What cannot be independently verified about any single vial is exactly why the tier below the line scores where it does.
Below the Line: Under 15
Everything past the line, no-prescription “tirzepatide” sites, vials labeled “for research use only,” unverified overseas sellers, gets scored as a single band, because they share the disqualifying trait: no clinician screens anyone, which zeroes out the two heaviest categories simultaneously. Oversight: zero, there is no clinician. Dispensing: near zero, no licensed pharmacy, no way to verify contents. Regulatory standing: near zero, “research use only” is a label used to dodge medical regulation, not a legitimate framework. Whatever points remain are cosmetic.
This is where the exercise stops being abstract. The medullary thyroid carcinoma and MEN 2 contraindication on the label is absolute [2], and a no-prescription site is that hazard in its purest form: a vial, a checkout, and nobody asking whether that family history applies, nobody preparing the dose correctly, nobody explaining how to escalate it without the GI effects landing hard. Under 15 is what “no oversight, no pharmacy” looks like once it is quantified.
The Variable Nobody Scores: The Molecule
The rubric above scores providers. It does not score tirzepatide. And on the evidence, tirzepatide would score at the top of its own class, which cuts the opposite direction from most compounds subjected to this kind of audit.
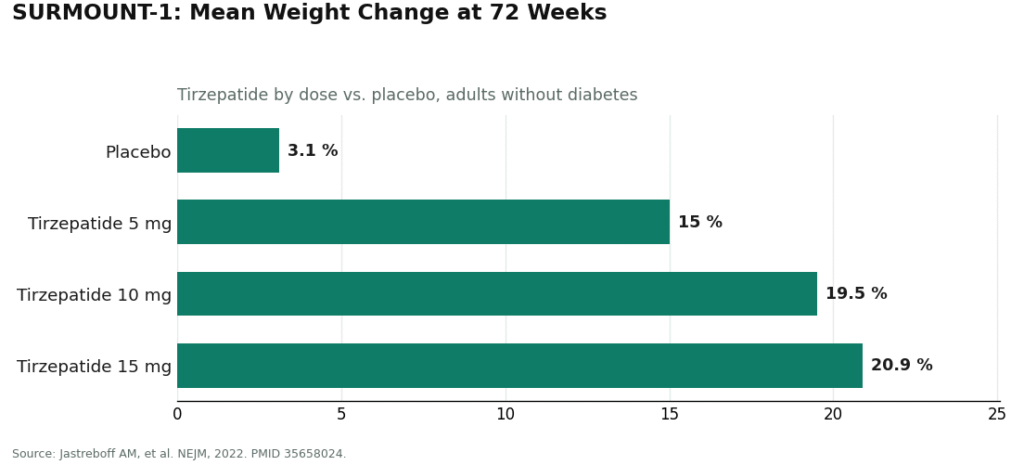
This is not a thin research file. In the SURMOUNT-1 trial, published in the New England Journal of Medicine, adults on once-weekly tirzepatide lost on average about 15.0% of body weight at 5 mg, 19.5% at 10 mg, and 20.9% at 15 mg over 72 weeks, against roughly 3.1% on placebo [1]. Large, durable, randomized-controlled-trial numbers, which is exactly why tirzepatide is FDA-approved as Zepbound for chronic weight management and Mounjaro for type 2 diabetes. Its mechanism, a dual GIP and GLP-1 receptor agonist rather than GLP-1 alone, is the documented pharmacology behind those figures [3]. Unlike the gray-market peptide world, “does the drug work” is not the open question. The provider score is the whole question, because the molecule already cleared its bar.
That is also exactly why oversight is weighted so heavily rather than less. A proven drug with a boxed warning is still a drug with a boxed warning [2]. A documented risk profile only protects a patient if someone actually reads it and screens against it. Scott Brunner, chief executive of the Alliance for Pharmacy Compounding, has put the honest boundary in public comments: compounding “should not be competition for FDA-approved drugs,” he has said, but rather “a secondary therapy designed to fill gaps in drug supply that FDA-approved drugs can’t fill.” Quoted here because he is a named source stating plainly what compounding is: a legitimate, regulated route, not a substitute identical to the branded drug. Every score in this piece lives in that space. A 95 is not a claim that compounded equals brand. It is a measurement of how accountable and well-supervised the access is.
Questions Worth Answering
Doesn’t a 95-to-under-15 spread just mean the rubric is rigged toward telehealth? Reasonable challenge. The rubric weights oversight and pharmacy dispensing heavily because those two things determine whether a dose is correct and whether anyone answers for it, and the absolute boxed-warning contraindication [2] is the receipt for why that weighting isn’t arbitrary. Re-weight the five categories any reasonable way and the licensed tier still beats the no-prescription tier, because the gray market scores near zero on the two heaviest categories regardless of how the rest gets shuffled. The large gap sits below the line. Above it, among licensed providers, the spread is small and the weighting argument is genuinely closer, which is why those scores sit within about a dozen points of each other.
Does a 95 mean compounded tirzepatide equals Zepbound? No. The score measures the accountability and quality of the supervised access, not the regulatory status of the product itself. The molecule is proven [1]. The compounded version is still not the branded product.
Why score the no-prescription tier at all, if it loses by seventy points? Because those sites are frequently the first thing people find, and leaving them off the page protects nobody. Scoring them transparently, stating the absolute contraindication and the absence of any licensed pharmacy plainly [2], is more useful than pretending they don’t exist or that they’re interchangeable with a licensed provider. Showing the gap on a shared scale does more work than just asserting it.
The bottom line of the exercise: the molecule already cleared its bar in the SURMOUNT trials. The only remaining variable worth measuring is who is standing between a patient and it.
What is tirzepatide and how does it work?
Tirzepatide is a once-weekly injectable that activates two hormone receptors at once, GIP and GLP-1, which is why it gets called a “dual agonist.” Those receptors regulate blood sugar, slow stomach emptying, and dampen appetite signals in the brain. It was FDA approved first as Mounjaro for type 2 diabetes in 2022, then as Zepbound specifically for chronic weight management in 2023.
Is the weight-loss data actually as strong as the marketing suggests?
The trial numbers hold up under scrutiny. In SURMOUNT-1, participants without diabetes lost around 20 percent of body weight on the highest dose over roughly 72 weeks, ahead of what earlier GLP-1 drugs showed in comparable trials. Individual results vary, weight tends to return after stopping the medication, and long-term cardiovascular outcome data is still being collected.
Is tirzepatide a GLP-1, or something else, and how does it compare to semaglutide?
Tirzepatide activates GLP-1 receptors, so it partly qualifies, but it also activates GIP receptors, which semaglutide does not touch. Semaglutide (Ozempic, Wegovy) is a pure GLP-1 agonist. Head-to-head data from trials like SURMOUNT-5 suggests tirzepatide produces greater average weight loss than semaglutide, though the side-effect profile for both is dominated by nausea and GI symptoms. Neither is the correct answer for every patient.
What side effects should someone realistically expect?
Nausea leads the list, particularly during dose escalation, followed by vomiting, diarrhea, constipation, and reduced appetite. Rarer but more serious concerns include pancreatitis, gallbladder disease, and a thyroid tumor signal flagged in animal studies, not confirmed in humans. Sourcing through a physician-supervised compounding pharmacy such as FormBlends, rather than a gray-market channel, at minimum puts a licensed provider in the loop to watch for these.
References
- Jastreboff AM, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine, 2022. PMID 35658024. Mean weight change roughly -15.0% (5 mg), -19.5% (10 mg), and -20.9% (15 mg) versus -3.1% placebo at 72 weeks. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Zepbound (tirzepatide) FDA-approved label: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2; warnings include acute pancreatitis and acute gallbladder disease; oral hormonal contraceptive interaction; most common adverse reactions are gastrointestinal. DailyMed (FDA label). https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=487cd7e7-434c-4925-99fa-aa80b1cc776b
- Farzam K, Patel P. Tirzepatide. StatPearls, NCBI Bookshelf. Dual GIP and GLP-1 receptor agonist, 39-amino-acid synthetic polypeptide.
- Kumari S. Peptides for Weight Loss: 8 Programs Ranked for 2026. LinkedIn (independent author). Ranks GLP-1/weight-loss programs on prescriber involvement, 503A pharmacy classification, purity-testing transparency, and clinical oversight; places HealthRX.com and FormBlends in the top tier.